

For more than four decades, HIV has remained one of the world’s most persistent public health challenges, reshaping societies, overwhelming health systems and deepening inequality across sub-Saharan Africa. Despite major progress in antiretroviral treatment and prevention, the epidemic has continued to claim lives in communities where poverty, stigma and limited access to healthcare intersect in dangerous ways.
Now, a new long-acting injectable drug is being introduced in parts of Africa, described by global health experts as one of the most significant breakthroughs in HIV prevention since the beginning of the epidemic. But as the world celebrates a scientific milestone, the reality on the ground remains shaped by fragility, funding cuts and human stories of survival—none more stark than that of Lianne.
Lianne was just 13 when AIDS took both her parents. She was forced to grow up faster than any child should.
After both her parents died from AIDS-related illnesses, she was left alone in Eswatini — a small southern African kingdom that still carries one of the world’s highest HIV infection rates. Suddenly orphaned, she became responsible not only for herself but also for her younger sister. There was no stable income, no government safety net and no realistic chance of staying in school.
Hunger made the decisions for her.
“I knew the dangers, but we needed to survive,” she says quietly.
Now 24, Lianne works as a sex worker in the outskirts of Mbabane, Eswatini’s capital. On good weeks, she earns less than £25. Some nights, she says, she returns home with almost nothing after paying for transport and food. Yet despite the risks she faces every day, she has continued because she sees no alternative.
For years, one thing gave her a measure of protection: access to free HIV prevention medication through mobile clinics funded largely by foreign aid. Then, almost overnight, those clinics disappeared.

The cuts to international assistance led to the closure of all 15 mobile HIV outreach clinics operating through local charities in Eswatini, according to health workers. For women like Lianne — among the communities most vulnerable to HIV infection — the consequences were immediate and terrifying.
A close friend and fellow sex worker recently contracted HIV after losing access to prevention medication. She later died.
“That scared all of us,” Lianne says. “It felt like we were abandoned.”
Now, however, a new medical breakthrough is offering a fragile sense of hope.
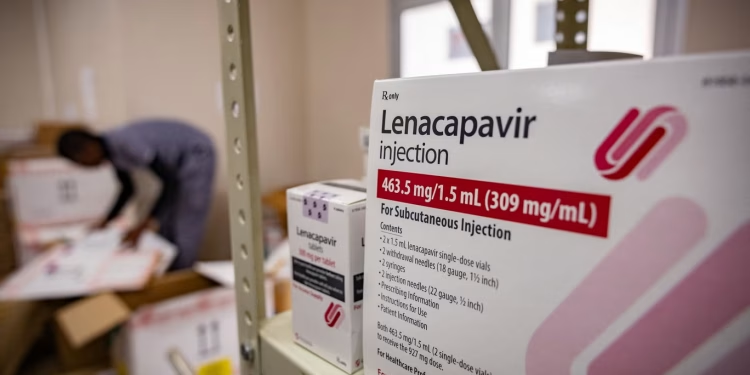
Inside a crowded clinic, Lianne rolls up her sleeve to receive a bright yellow injection of lenacapavir, a revolutionary HIV prevention drug that scientists and global health officials believe could change the course of the epidemic.
“This is protection,” she says, exhaling with visible relief. “This means I can live.”
The twice-yearly injection has been described by the head of UNAIDS as “the closest thing we have to a vaccine” against HIV. Clinical trials showed it offers near-total protection against infection, marking one of the most significant advances in HIV prevention since antiretroviral therapy transformed AIDS from a death sentence into a manageable condition.
For countries such as Eswatini, where HIV has shaped generations, the drug’s arrival carries extraordinary significance.
Once known as Swaziland, Eswatini was long regarded as the epicentre of the global HIV epidemic. At its peak two decades ago, the country recorded around 21,000 new infections annually. Although that figure has fallen sharply — to roughly 4,000 new infections in 2023 — the virus still casts a shadow over daily life.
Around one in four adults between the ages of 15 and 49 are living with HIV, according to the latest data from the U.S. Centers for Disease Control and Prevention.

Entire communities still carry memories of funerals that became heartbreakingly routine during the worst years of the epidemic. Many young people grew up without parents. Others became caregivers while still children themselves.
Lianne belongs to that generation.
She remembers watching her parents become weaker and thinner before they died. Afterward, survival consumed everything.
“There was no money for school,” she says. “Sometimes we had no food at home. I had to think about my sister.”
Another young woman waiting at the clinic, 17-year-old Arianna, tells a strikingly similar story. After her mother died, she fled an abusive home and eventually turned to sex work to survive.
Trying to access daily HIV prevention pills, known as PrEP, was almost impossible, she says. Public health facilities often exposed women like her to judgment and humiliation. Even transport costs could be overwhelming.
“You go there and people look at you differently,” she says. “Sometimes you do not even have money to travel there every day.”
For women living in poverty and facing social stigma, a twice-yearly injection could remove enormous barriers to protection.
“That is why I came today,” Arianna says. “This can save our lives.”
The rollout of lenacapavir is being hailed by global health officials as a historic turning point. Supported by the Global Fund to Fight AIDS, Tuberculosis and Malaria, alongside international partners including the U.S. government, the initial programme aims to deliver the injections to millions of people most at risk.
Eswatini became the first country in the world to begin distributing the drug as part of the initiative.

“This is a defining moment in the AIDS response,” says Dianne Stewart of the Global Fund. “For decades, life-saving innovations reached wealthy countries first while poorer nations waited years. This time, we are trying to change that.”
That contrast remains painful across much of sub-Saharan Africa.
When antiretroviral drugs first became available in Europe and North America during the late 1990s, many African countries waited nearly a decade before treatment became widely accessible. Millions died during that delay.
Health advocates fear history could repeat itself if lenacapavir is not distributed rapidly and equitably.
The drug currently costs as much as $24,000 per year in wealthy countries, although international agreements have significantly lowered prices for low-income nations participating in the rollout.
Still, concerns are growing that access remains far too limited.
At a Médecins Sans Frontières clinic outside Mbabane, doctors say demand has already exceeded supply. The clinic reportedly received only 50 doses during the initial phase of distribution and has been forced to turn patients away.
“We know this drug can transform HIV prevention,” says Dr. Diojki Bahati, the organization’s country lead. “But the current scale is nowhere near enough.”
Global health experts warn that isolated or uneven access could weaken the overall impact of the breakthrough. HIV remains a global epidemic, and infection rates are climbing in several regions, including parts of Latin America where lenacapavir has yet to be fully licensed or procured.
“We learned during Covid that you cannot protect one part of the world while leaving others behind,” Stewart says. “Infectious diseases do not respect borders.”
UNAIDS estimates that around 20 million people need access to HIV prevention medication in the coming years if the world hopes to end AIDS as a public health threat by 2030.
Current plans, however, aim to reach only a fraction of that number by 2028.
The timing could hardly be more critical.
At the beginning of 2025, global health agencies believed the world was on course to bring the AIDS pandemic under control within the decade. But sweeping cuts to foreign aid budgets by the United States, Britain and several European countries disrupted HIV programmes across Africa almost immediately.

Testing campaigns slowed. Prevention programmes were suspended. Community outreach teams disappeared.
David Maseko, who works with HealthPlus for Men — an organization supporting vulnerable communities including LGBT+ people and sex workers — says the closures created dangerous gaps in care.
“There are now many people who are off treatment and off PrEP,” he says. “We are even struggling to continue community testing.”
The consequences extend far beyond immediate infections. Health experts warn that interruptions to HIV treatment can also increase drug resistance, creating strains of the virus that are harder and more expensive to treat in the future.
According to modelling by researchers and humanitarian organizations, continued funding cuts could lead to millions of additional infections and deaths globally over the next decade.
That would also create enormous economic costs.
Carmen Pérez Casas, of the global health initiative Unitaid, says preventing infections through lenacapavir would ultimately be far cheaper than treating new HIV cases for life.
In 2024 alone, there were approximately 1.3 million new HIV infections worldwide. Providing lifelong antiretroviral therapy for those infected could cost billions of dollars over time.
“Prevention is not only lifesaving,” Pérez Casas says. “It is economically essential.”
Back inside the Eswatini clinic, the emotional weight of the moment is impossible to miss.

Young women sit shoulder to shoulder, waiting nervously for their injections. Some scroll through phones. Others stare silently at the floor. Many carry histories marked by violence, poverty and loss.
Yet for a brief moment after receiving the injection, relief softens the fear.
Lianne smiles faintly as a nurse presses cotton against her arm. She knows one injection cannot erase the hardships surrounding her life. Poverty remains. Hunger remains. The dangers of her work remain.
But for the first time in months, she feels protected.
“We are begging the world not to forget us,” she says before leaving the clinic. “If the funding disappears, people like us will die. We need help to survive.”
















{kind=link}
Discussion about this post